Abstract
Introduction: We investigated the risk factors of poor outcomes in MIS short fusion for adult spinal deformity (ASD).
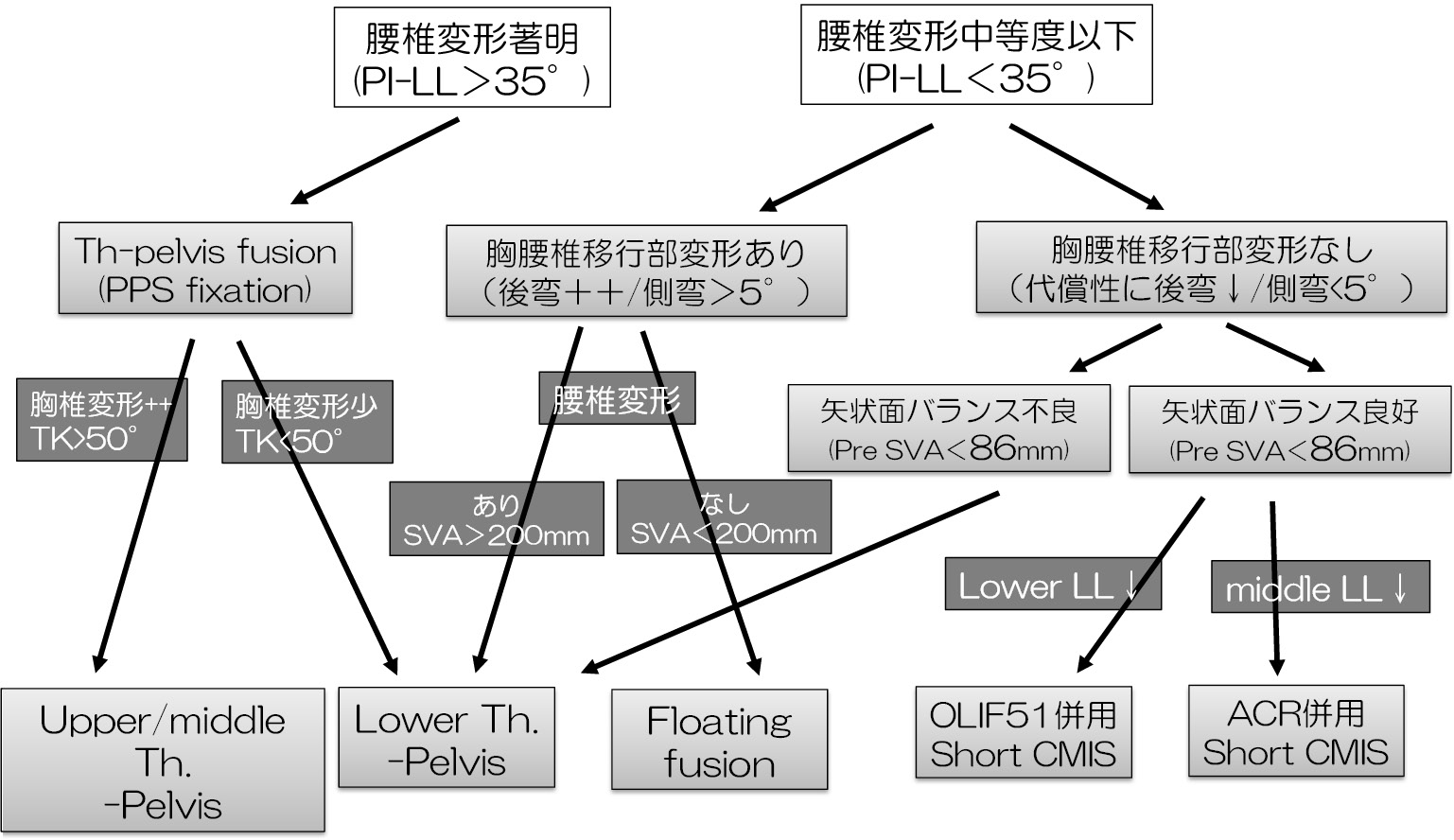
Subjects and Methods: The study included 82 patients with adult spinal deformity (ASD) who had undergone MIS-short fusion using MIS techniques such as LLIF, ACR, and PPS at T12 or below, and who had been able to be followed up for at least 2 years. The average age was 73.7 years, and the average follow-up period was 35.5 months. The definition of poor results was final SVA > 50 mm or the development of PJF/DJF. Firstly, we divided the patients into Group G (final SVA≤50 mm) and Group P (final SVA>50 mm), and examined the femoral bone mineral density, number of fixation ranges, HU value (UIV), various parameters, GAP score, ODI, and walking speed. Next, we examined the same items in two groups: Group JF (with JF) and Group NJF (without JF).
Results: In the first analysis, there were no significant differences in age, gender, bone mineral density, or HU value, and the fixed range was significantly shorter in the G group. In the G group, the preoperative and postoperative LL were significantly larger, the PI-LL was significantly smaller, and the preoperative and postoperative SVA were significantly smaller. In addition, there were significant differences in the RLL (LL-ideal LL) and RSA (global tilt (GT) -ideal GT) in the GAP score. There was no significant difference in gait speed, and the postoperative ODI was significantly smaller in Group G. In multivariate logistic regression analysis with the final-SVA>50 mm as the objective variable, only the preoperative SVA was detected as a risk factor. Similarly, univariate and multivariate analyses were performed on the JF and NJF groups, and the risk factors for JF were found to be GAP score.
Conclusion: In MIS short fusion for ASD, preoperative SVA is important for final SVA, and the importance of GAP score in the occurrence of JF was suggested.