Abstract
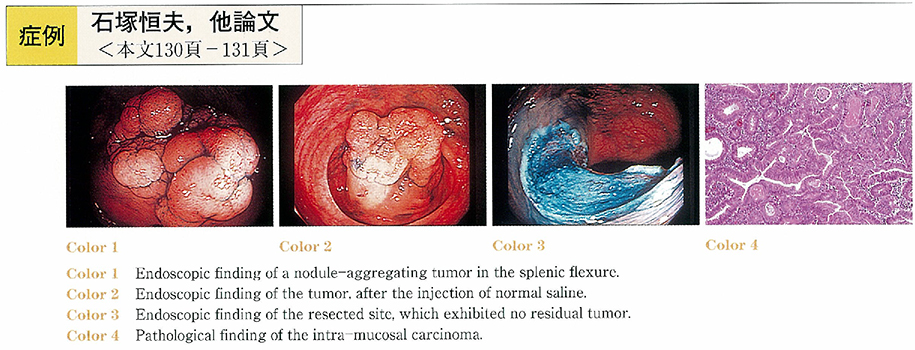
The case was a 53-year-old male who complained of a fecal occult blood. Colonoscopy revealed a nodule-aggregating tumor of 49 mm in diameter in the splenic flexure. In supine position, it was not possible to have the entire view of the lesion. However, in left lateral position, it was possible to have an entire view of the lesion. We injected normal saline containing epinephrine into the submucosa adjacent to the oral side of the tumor. That procedure resulted in a protrusion of the oral side of the tumor. Subsequently, the anal side of the tumor was pressed down with the base of the snare, which enabled a successful snaring of the lesion. After first resection, a small part of the tumor remained at the oral side. The residual tumor was resected completely by the second snaring. Histologically, the tumor was a tubulo-villous adenoma containing the areas of well-differentiated adenocarcinoma not invading to the submucosal layer. Colonoscopy was repeated three months after the resection, which revealed no residual or recurrent tumors.
It has been reported that the maximum size of flat colorectal tumor, in which en bloc endoscopic mucosal resection can be performed, is 30mm in diameter. We present a case of a large flat tumor totally resected endoscopically almost in one piece.